Angioplasty vs Bypass Surgery — How the Right Treatment is Chosen
When a patient is found to have significant blockages in their coronary arteries, the question inevitably arises: is angioplasty (with stenting) or bypass surgery the right treatment? Both are effective — but they work differently, have different recovery times, and suit different patients. Understanding the factors that guide this decision helps patients and families participate meaningfully in the conversation.
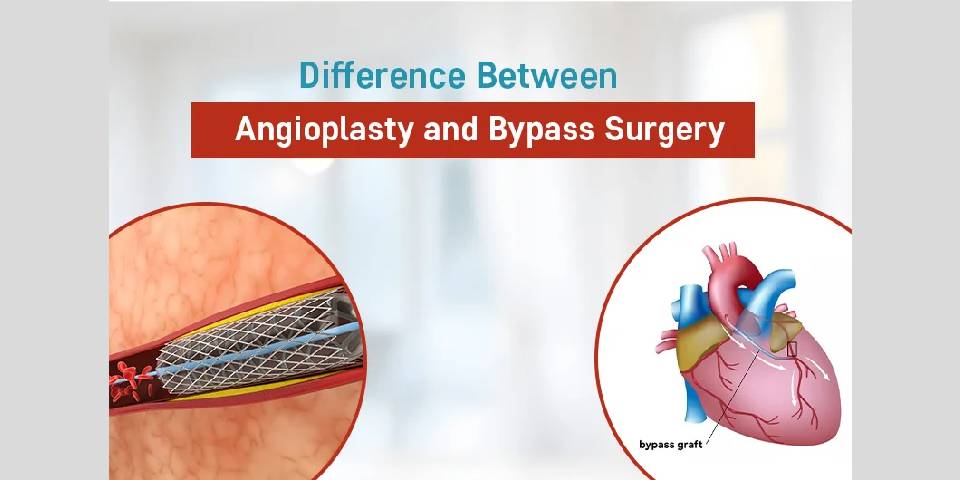
What is the difference?
| Coronary angioplasty (PCI) | A catheter is guided through a blood vessel to the blockage. A balloon is inflated to open the artery and a stent is placed to keep it open. No chest incision required. Recovery in days to weeks. |
| Bypass surgery (CABG) | The chest is opened. A blood vessel taken from the leg, chest wall, or arm is used to create a new route (bypass) around the blocked artery. Requires a heart-lung machine. Recovery in 6 to 12 weeks. |
How is the decision made?
The choice is not arbitrary — it is guided by well-established international criteria based on your angiogram findings, overall heart function, and coexisting conditions. The key factors are:
Number and location of blocked arteries
- Single vessel disease (one blocked artery) — angioplasty is almost always preferred
- Two vessel disease — usually angioplasty, depending on which arteries are involved
- Three vessel disease — surgery may be preferred, especially in diabetic patients
- Left main artery disease — historically favoured surgery, but angioplasty is now a valid option for many patients with left main disease, particularly those at high surgical risk
The SYNTAX score — measuring complexity
The SYNTAX score is an internationally validated system that gives each blockage a numerical score based on its location, length, calcification, and complexity. A low SYNTAX score favours angioplasty; a high score favours surgery. Dr. Bhishma Chowdary calculates the SYNTAX score for every patient requiring a revascularisation decision.
Heart muscle function
Patients with significantly reduced ejection fraction (heart pumping strength below 35%) may benefit more from surgery in terms of long-term survival — particularly when combined with other surgical procedures such as valve repair.
Diabetes
Diabetic patients with triple vessel disease have shown better long-term outcomes with bypass surgery in large trials. For single or double vessel disease, angioplasty remains appropriate regardless of diabetes status.
Surgical risk
Age, frailty, lung disease, kidney disease, prior cardiac surgery, and other conditions all affect the risk of open-heart surgery. For patients at high surgical risk, angioplasty may be the safer option even when anatomy might otherwise favour surgery.
When angioplasty is preferred
- Single or double vessel disease
- Suitable anatomy (SYNTAX score below 22)
- High surgical risk patients
- Patient preference for avoiding major surgery and faster recovery
- After a heart attack requiring urgent revascularisation (primary PCI)
- When a previous bypass graft has failed and re-do surgery carries high risk
When bypass surgery may be better
- Triple vessel disease — particularly in diabetic patients
- Left main artery disease with high SYNTAX score
- Need for simultaneous valve surgery or other cardiac procedures
- Anatomy unsuitable for complete stenting
- Young patients with long life expectancy where surgical graft durability is an advantage